I wasn’t going to revisit this topic, but when the biggest debate in the Clinic is over Froome’s nationality, it seems like a good time to summarize what I’ve learned about his salbutamol case since he was exonerated.
After I wrote a summary/critique of the Froome case, several months ago, Daren Austin, the GLAXO researcher who convinced WADA/UCI that Froome’s urinary salbutamol level could have occurred without taking more than the maximum allowed amount, got in touch with me, and discussed some general aspects of his work. He asked that I not share his personal communications, and he would not discuss the specifics of Froome’s case, including his salbutamol levels during other stages of the 2017 Vuelta, which I really wanted to know. However, he did make a couple of very general points about salbutamol, which I believe I can share here without violating the spirit of my agreement.
First, he noted that most scientists assumed, incorrectly, that drug concentrations in the urine follow a Gaussian or normal distribution. That is, if you give a group of subjects a fixed dose of salbutamol—or if one subject takes the same dose at different times—the urinary levels at some time after the dose will be distributed as a typical Bell curve. From such a distribution, one can determine a mean and standard deviation, and from these values, one can estimate the probability of any particular urinary level occurring by chance.
For reasons I won’t get into here, usually the distribution is not normal, but log normal. That is, it’s the logarithms of the values that are normally distributed. This is critical to Froome’s case, because in a lognormal distribution, the actual values—as opposed to their logarithms—are skewed to the right. This means that the probability of very high values is considerably greater than one would estimate based on a normal distribution.
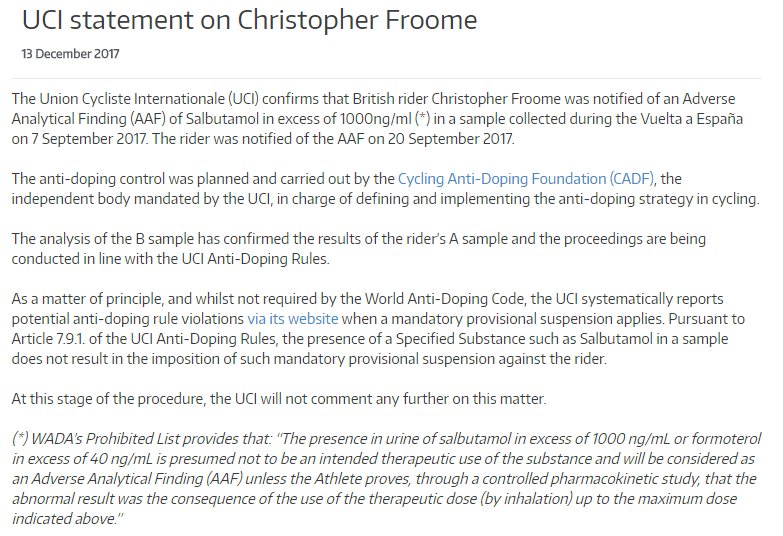
The second key point is that there are different kinds of inhalers; in particular, there’s a distinction between the MDI, measured dose inhaler, and the Diskus, in which dry powder is inhaled. A study that was published about a year ago showed that the amount of salbutamol getting into the circulation was 50-100% greater when the MDI was used than when the Diskus was used, despite the fact that the nominal dose inhaled was the same. This is also critical to Froome’s case, because while he used the MDI, some of the studies on which WADA based its criterion used the Diskus. In other words, while Froome may have inhaled no more than the maximum allowed dose of 800 ug, as determined by the MDI, that dose could have been equivalent to much more than the 800 ug dose used by WADA in its Diskus studies.
Austin’s argument was that when these two factors—and several others that I will not get into here—are taken into account, Froome’s salbutamol level had a reasonable probability of occurring despite his not taking more than the maximum allowed dose. Since he didn’t specify what this probability was, and I’m not privy to Froome’s other values, I can’t judge how valid this conclusion is. I did go back and re-evaluate all the published WADA studies assuming a lognormal distribution. I was able to show that their values generally did follow this distribution, in agreement with Austin, but I also established that for most of these studies, the actual mean and SD values, based on a lognormal distribution, still indicated that the probability of Froome’s value was quite low. In 7/8 studies, the probability was < 3%, and the weighted mean of all the studies was about 1.5%.
This probability would be a problem for a test applied to a large number of subjects, as the risk of a false positive would be relatively high, and no doubt this is why WADA has suggested it will lower the maximum amount allowed to be inhaled. Probably the only reason there haven’t been more salbutamol positives in the past is because athletes generally have not taken the full allowed dose. However, as applied only to Froome, this probability indicates that his value—based simply on the lognormal argument, nothing else-- would be quite unlikely to result from an allowed dose. I'll also add that i personally never emphasized the standard deviation argument, anyway, but just noted that out of nearly 200 published samples, none exceeded Froome's value, assuming the correction for urine specific gravity was allowed. This point holds regardless of the nature of the distribution.
As for the inhaler effect, while it’s true that some WADA studies used the Diskus, other studies used the MDI, so their results should be relevant to Froome’s level. In fact, comparison of the results of studies using the two types of inhalers generally does not support the conclusion that the amount of salbutamol getting into the system with the MDI is much greater than with the Diskus. That is, there are studies using the MDI at a given dose which result in urinary levels very similar to those observed when the Diskus was used to inhale the same dose. These studies directly contradict the result of the study that Austin pointed out to me. I don’t know how to resolve this discrepancy, except to note that the latter study only measured amounts of salbutamol in the blood, not in the urine. This shouldn’t matter, but FWIW, there’s no study I’m aware of that compares urinary levels of salbutamol following inhalation with MDI vs. Diskus.
Though Austin didn’t say so, I suspect that one reason WDA/UCI did not publish the report is because it was embarrassing to them. They should have known about the lognormal distribution—I should have known this, too, and that is mea culpa,though again, it doesn't really affect the argument I was making—and they should have known about the difference between the inhalers, though that study was only published shortly before the 2017 Vuelta. They have not come out of this looking good.
Another important factor, noted by UCI when it announced its decision, was the effect of dehydration. Several studies suggest that dehydration can increase urinary levels, not simply because the urine was more concentrated, but even taking into account correction for this concentration. However, a crucial question becomes, how dehydrated was Froome on the day of his positive test? While we don’t know—and I don’t think he himself or his legal/scientific team knows--we do know what his urinary specific gravity (USG) was, and I found a couple of studies that relate USG to body mass. Based on these studies, it appears that Froome had a maximal body fluid loss of 3%. This is in agreement with other studies, discussed earlier in this thread, that indicate that greater loss of body fluid is associated with performance deficits. In fact, most evidence indicates that performance deficits occur at losses of > 1.5- 2.0%, so I would think it unlikely that Froome’s loss exceeded this. When Petacchi tested positive for salbutamol, he had an even greater USG, suggesting an even greater fluid loss. This is quite difficult for me to understand, given he not only won the stage, but on a flat sprint, where the power loss would not at least be partially compensated for by a lower body weight, as in the case of the climbing finish that Froome faced. In any case, it seems that dehydration would have a limited effect on Froome’s levels. One of the studies being touted as relevant to Froome’s levels used a body fluid loss of 5%, and that almost certainly was far more than Froome’s loss.
Austen told me that he was publishing a couple of papers relevant to the salbutamol criterion, though as far as I know, they haven’t appeared yet. Absent the actual report, which apparently will never be released despite promises from various parties, it’s not possible to judge how strong the case was for letting Froome off. But based on what data I’ve seen, I’m pretty sure that the probability of his level occurring without taking more than the allowed amount was still fairly low. When Austin’s role was first announced in the media, a figure of 10% was mentioned, which sounds shockingly high, but which still indicates that he would more likely than not have taken more than the allowed amount. I suspect that what probably carried the day was the argument that he would never intentionally dope with salbutamol during a race when he knew he would be tested. So even a relatively low probability would be higher than the probability of the alternative.

")