Either I've been giving people more credit than they deserve, or you are giving them less.
For me, this is the key statement in the whole discussion of aerosols vs. surfaces. Much of what KB says makes sense to me IF many/most people don't wear masks and sanitize their hands regularly. My assumption--and I've been lucky enough not to have to test it yet--is that people in food markets will be extra cautious, because this is the one place where everyone is touching things, the same things everyone else is touching, things that will go into your mouth. I can't imagine people would pick up anything w/o either wearing disposable gloves, or sanitizing their hands immediately after, but maybe this is not the case.
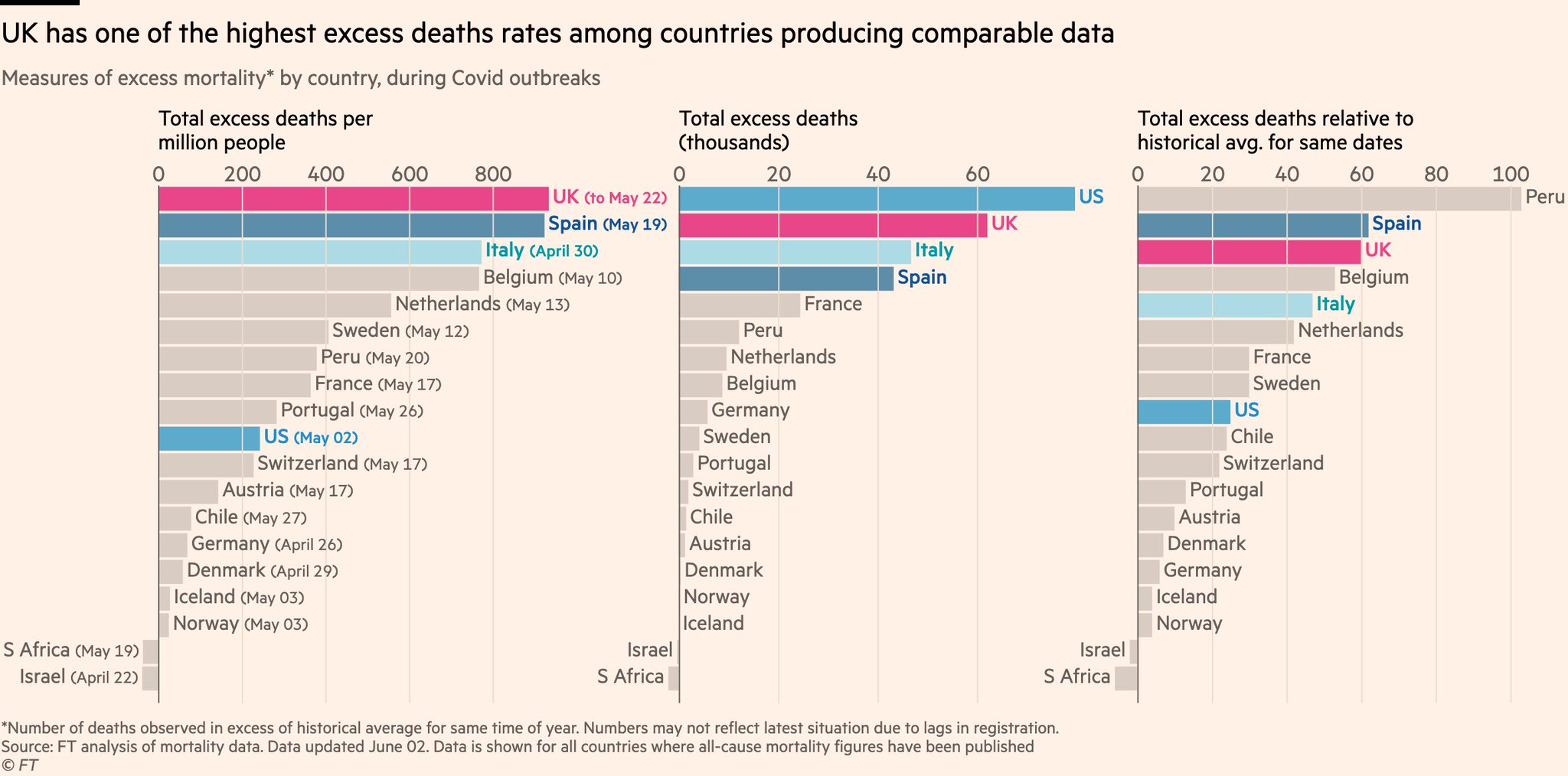
According to these numbers one could argue that the US has done quite well compared to many countries.
The U.S. looks good when you compare it to the small handful of countries that have the highest mortality rates in the world. It has the eighth highest mortality rate of countries with a population of > 10 million (there are more than 80 of them, which puts the U.S. in the 90th percentile), and has the second highest case rate in this group. Sure, you can argue that some countries are under-reporting, but this doesn't change the general conclusion.
No, the U.S. has not done well.
I think the problem in the US is that there is no clear national strategy, and that the infection is in different stages in different states, which makes renewed spread from 'later' states to 'earlier' states possible.
Sure, but why is there no clear national strategy? And why are the highest case and death rates in Western countries, while SE Asia, Taiwan, S. Korea, and "socialist" Norway are doing so well? A lot of America's problem is that pandemics are best handled by people with a strong sense of the collective. Individualism has its strengths, but it doesn't help much when a non-discriminating virus is sweeping the land. The most successful countries locked down early, did lots of testing, and were aggressive in contact tracing. The U.S. has basically taken a half-assed approach to these.
This head of IC, has said some strange things on RAI (Italy):
Il primario del San Raffaele di Milano, direttore della terapia intensiva: "Sono tre mesi che sciorinano una serie di numeri che hanno evidenza zero"…

www.repubblica.it
Basically, he says that the virus has changed, that the viral loads in new patients are much lower than before. But, it's unclear why he claims that and what proof he has.
It frankly reads as someone citing flimsy evidence to push a political view (end lockdowns). The way to determine if the virus has become less lethal or infective is sequence analysis, not the amount of load in recent cases.