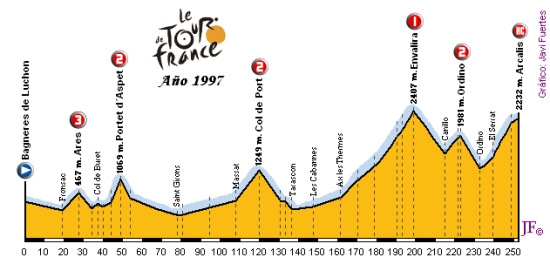
After 7 3/4 hours in the saddle, Jan breaks away solo on the final stretch to the summit (10.6km at 7.1 percent) and wins by 67 seconds. Just the kind of climb that suited Ullrich. I have seen more disturbing performances at the tdf.Race Radio said:There is nothing in Jan early career that would indicate what happen on the Arcalis was possible. Nothing. It was one of the more disturbing displays in the sports history

Jan Ullrich
Page 31 - Get up to date with the latest news, scores & standings from the Cycling News Community.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
- Apr 20, 2012
- 6,320
- 1
- 0
You mean for a non - climber a suited climb? This was as bad@ss as Riis on Hautacam.Bratam said:After 7 3/4 hours in the saddle, Jan breaks away solo on the final stretch to the summit (10.6km at 7.1 percent) and wins by 67 seconds. Just the kind of climb that suited Ullrich. I have seen more disturbing performances at the tdf.
Lol:
http://ftp.cyclingnews.com/results/archives/tour97/stage10.htmlBut insiders such as American Lance Armstrong, recovering from cancer and looking to race again for the Cofidis team, said the young German's talent has long been evident.
``It's not so surprising. He's a talened young guy who was world champion as an amateur (in 1993). He could win many more Tours,'' Armstrong said after the 10th stage, second in the Pyrenees, which Ullrich won by a one minute eight seconds margin.
At 23, Ullrich is the same age as Frenchmen Jacques Anquetil and Bernard Hinault, both five times winners, and their compatriot Laurent Fignon, twice a victor, were when they won their first Tours.
Ullrich named Spain's Miguel Indurain, who also won the Tour five successive times until he was succeeded by Riis in 1996, as his idol.
Such of soft stage.
- Apr 7, 2011
- 4,887
- 465
- 16,580
Fearless Greg Lemond said:Just look at this page:
http://www.researchgate.net/profile/Giovanni_Grazzi/
and note the co-researchers/reviewers. A nice band of brothers - and one sister who is now at Astana - if you ask me.
The genie was long out of the bottle, and, I do belief the Freiburg dottores were able to read up.
Claiming that Ullrich worked with obe of them in 1997 is wrong nevertheless.
- Aug 13, 2010
- 3,317
- 0
- 0
I dunno... When Riis rides away from everyone while riding tempo - that is pretty brutal.Fearless Greg Lemond said:This was as bad@ss as Riis on Hautacam.
Yeh, good question.Zam_Olyas said:On a level playing field who could have won those tours then?
- Aug 13, 2009
- 12,854
- 2
- 0
Bavarianrider said:Ullrich did NOT work with one of this doctors when he won the Tour!
If you want to split hairs yes, Jan started working with Checchini in 2002. When he won the Tour he he used Heinrich and Schmid. No surprise that the next year he is right on Armstrong's wheel.
None of that changes what I wrote.
thehog
BANNED
- Jul 27, 2009
- 31,285
- 2
- 22,485
Race Radio said:If you want to split hairs yes, Jan started working with Checchini in 2002. When he won the Tour he he used Heinrich and Schmid. No surprise that the next year he is right on Armstrong's wheel.
None of that changes what I wrote.
Race man, calm down.
Ullrich was pure class. It was obvious to see. Extremely talented rider.
You need to take your Sky/Garmin shades off.
Ullrich maybe not the best climber ever but darn good. Was better than Armstrong if both clean.
- Jan 27, 2010
- 921
- 0
- 0
Race Radio said:Not never....one season. 2001.
...
Using your numbers. If Jan's HCT for 2001 was 43, and most other riders maxed out their HCTs at say 49, that is 6 pts of HCT that Ulle was behind all of them; about 13%. That is a lot to make up even for 2 bags of your own blood...and he still finished 2nd to Lancey. I am sure everyone was using Cortisone, IV rehydration and the top 10 had access to Blood re-infusions leveling the playing field.
Stands to reason that in 2001 he was a pharmaceutical underdog, without use of 'super-responder' EPO possibilities/excuses and performed very well. The super-responder explanation cannot apply for that year. What does that say about his abilities then? Surely he is better than peoples negative and dismissive comments "...fat climber, couldn't keep up, EPO responder..." It would appear that Jan tried to limit his drug use in 2001 and when Lancey smoked him day after day, climb after climb he just said "scr$w this, I'm doping full gas next year."
Was 2001 the year that he trained well, was lean and his capabilities shone through relative to the other dopers of equal or superior PED use? What are the potential holes in that theory?
I think he also trained hard in 2000. I can recall the lead up to the 2000 olyimpics and there was talk that Ullrich had been busting his backside and was in incredible shape. The 1st EPO test had also just become available in time for the Olympics.Neworld said:Was 2001 the year that he trained well, was lean and his capabilities shone through relative to the other dopers of equal or superior PED use? What are the potential holes in that theory?
Ullrich went on to win Gold in the Road Race. In the Time Trial, Ullrich and Armstrong were the the last two riders and Ullrich beat Armstrong by more than 30 seconds and should have taken his 2nd Gold medal. However, a certain Viacheslav Ekimov had raced more than an hour earler in the day and had managed to beat Jan by eight seconds to win Gold. As it turns out, Ekimov had significant wind behind him and by the time Jan and Lance were on the blocks the wind had shifted against them. The experts had estimated that Ekimov had more than a 30 second wind advantage over the later riders.
- Jul 15, 2010
- 464
- 0
- 0
Bratam said:I think he also trained hard in 2000. I can recall the lead up to the 2000 olyimpics and there was talk that Ullrich had been busting his backside and was in incredible shape. The 1st EPO test had also just become available in time for the Olympics.
Ullrich went on to win Gold in the Road Race. In the Time Trial, Ullrich and Armstrong were the the last two riders and Ullrich beat Armstrong by more than 30 seconds and should have taken his 2nd Gold medal. However, a certain Viacheslav Ekimov had raced more than an hour earler in the day and had managed to beat Jan by eight seconds to win Gold. As it turns out, Ekimov had significant wind behind him and by the time Jan and Lance were on the blocks the wind had shifted against them. The experts had estimated that Ekimov had more than a 30 second wind advantage over the later riders.
One thing I found funny was that Big Mig made a comment that he would comeback if Ekimov would win another gold. Seeing how comebacks can go, he was wise not to stay to his word.
Lets not forget that Ekimov was one of only two riders who defended Armstrong right up until the end. Rather than going quiet, Ekimov was a staunch defender of Armstrong and was in complete denial about all doping allegations at USPS right up until release of the USADA reasoned decision. Ekimov must look like the biggest ****wit this side of Austin, Texas right now. Rather than being ousted from Cycling world, Ekimov now heads the Katusha team. What a joke !Zweistein said:One thing I found funny was that Big Mig made a comment that he would comeback if Ekimov would win another gold. Seeing how comebacks can go, he was wise not to stay to his word.
No surprise that nowadays Ekimov refuses to answer questions that he was doped throughout his career.
- Sep 30, 2011
- 9,560
- 9
- 17,495
Zam_Olyas said:On a level playing field who could have won those tours then?
Will anyone tempt to answer this?
- Aug 6, 2009
- 2,112
- 7
- 11,495
It seems as if some of you are having a difficult time coming to grips with Race Radio stating that Ullrich would, like Armstrong, have been nothing but a Classics specialist if not for the doping. Let's go over some other issues-
1) Just because a couple of riders and cycling analysts said he was the best talent of his generation yet never speculated as to why (which one has to with the type of doping being practiced at the time), that doesn't take into account his absolutely abysmal form the large majority of the time he raced.
2) He really only had one great day in the mountains at the Tour, and that was in 1997. The rest of his career was, aside from his performances at one Vuelta and the Olympics, potential that was spoken about ad nauseum but never fully realized.
3) He was hounded out of the sport, yet he could have served a suspension with plenty of time to come back and redeem himself. He chose not to.
4) No one knows what his true potential might have been because he probably did not race clean those two years at Telekom in 1996-1997 when he first became noticed on the international scene. And if he was doping as an amateur, that muddies the waters even further.
Since Ullrich has stated he will NOT go into any details over his doping history, we are left to conjecture. I believe more people are willing to exaggerate his natural talents only because he didn't have a personality similar to Armstrong, just as Indurain gets a pass for the same reason.
All three have one thing in common-ridiculous performances that announced to the cycling world "I'm here, I'm on dope, and no one can stop me"-Ullrich at Arcelis, Indurain's time trial from Tours to Blois, and Armstrong at Sestriere. I see no difference between these three performances.
Judging from Armstrong's trajectory as a Tour Juggernaut, I find it very easy to come to the same conclusion as Race Radio about Ullrich, with the exception that I nor anyone else here is privy to his information, which may I remind his current crop of doubters on the forum, is about as good as it gets and in my opinion beyond reproach.
That along with the fact that over the years RR has never been given to fits of hyperbole, has maintained an unprecedented level of decorum even when scurrilously attacked, and has shared more in-depth information for our benefit than just about anyone else bar none, leads me to believe his assertion about Ullrich is correct.
1) Just because a couple of riders and cycling analysts said he was the best talent of his generation yet never speculated as to why (which one has to with the type of doping being practiced at the time), that doesn't take into account his absolutely abysmal form the large majority of the time he raced.
2) He really only had one great day in the mountains at the Tour, and that was in 1997. The rest of his career was, aside from his performances at one Vuelta and the Olympics, potential that was spoken about ad nauseum but never fully realized.
3) He was hounded out of the sport, yet he could have served a suspension with plenty of time to come back and redeem himself. He chose not to.
4) No one knows what his true potential might have been because he probably did not race clean those two years at Telekom in 1996-1997 when he first became noticed on the international scene. And if he was doping as an amateur, that muddies the waters even further.
Since Ullrich has stated he will NOT go into any details over his doping history, we are left to conjecture. I believe more people are willing to exaggerate his natural talents only because he didn't have a personality similar to Armstrong, just as Indurain gets a pass for the same reason.
All three have one thing in common-ridiculous performances that announced to the cycling world "I'm here, I'm on dope, and no one can stop me"-Ullrich at Arcelis, Indurain's time trial from Tours to Blois, and Armstrong at Sestriere. I see no difference between these three performances.
Judging from Armstrong's trajectory as a Tour Juggernaut, I find it very easy to come to the same conclusion as Race Radio about Ullrich, with the exception that I nor anyone else here is privy to his information, which may I remind his current crop of doubters on the forum, is about as good as it gets and in my opinion beyond reproach.
That along with the fact that over the years RR has never been given to fits of hyperbole, has maintained an unprecedented level of decorum even when scurrilously attacked, and has shared more in-depth information for our benefit than just about anyone else bar none, leads me to believe his assertion about Ullrich is correct.
- Jul 27, 2010
- 5,121
- 884
- 19,680
look, every DS in the 90/00's understood the Hct/Vo2 formula. They also understood that when your body suddenly has 20% more RBC that unless you have muscles to absorb that additional oxygen that it is wasted. One thing Jan had was muscle in all the right places. Lance had this as well. Surprisingly Pantani also had this. Roberto Pregnolato, Marco Pantani's soigneur. said he was the most densely muscled rider he ever worked with.
20%?! In the nineties, maybe, but not after the EPO test. The typical transfusion of 500 ml. is about one-third of that. And during a GT, much of the transfusion goes just to reverse the normal decline in HT, so I don’t see a big issue with the extra oxygen being absorbed. The fact is that a typical racer has a natural HT about the same as a typical non-racer—low to mid 40s—but training results in a large increase in mitochondria and in the activity of certain aerobic enzymes. I don’t see how a 5-10% increase in oxygen intake is going to be wasted. If you really buy into the theory that more muscle mass is necessary to make use of increased oxygen intake, you would have to accept as a corollary that a rider without the benefit of increased oxygen intake would do worse than normal, because of all that muscle sitting idle.
As for having “muscle in all the right places”—I would assume any GC contender fits this description, and to the extent he does, is going to do very well relative to the competition all-clean or all-doped. This is beginning to sound like the “Lance had a heart three times larger than anyone else” arguments. Speculation based on little hard evidence to support a pet theory.
Take two riders with identical Vo2. One has a natural Hct of 41 the other is at 48. Both can boost their Hct to 50......which one gets the most benefit? How does a rider who gets a 2% boost in Vo2 compete with one who gets a 13% boost?
Definitely true, but it undercuts your argument that Ulle’s success was due in large part to having the right doctors. If you have a relatively low HT, and are operating pre-passport where anything up to 50% is allowed, you are going to benefit more from blood boosting regardless of who your doctor is. But based on the information I've seen, neither Ulle's nor LA's HT was exceptionally low. As I said before, an average HT is in the low forties, which suggests about half the peloton had the same advantage as these two, or even greater.
Now add in the cocktail of drugs, under expert supervision, that when administered correctly and on schedule add lean muscle mass that can put that additional RBC to good use.
Are there any scientific studies supporting this? I didn’t think so.
No doubt, some programs are better at adding muscle than others. But anyone taking these substances is going to be capable of more power, regardless of whether he's blood boosting or not. And conversely, anyone blood boosting is going to be capable of more endurance, regardless of whether he's adding muscle or not. You seem to be implying that the program was tailored to coordinate the increase in muscle mass with an increase in oxygen intake. I doubt very much that the doping doctors were trying to do this, or that in fact one could do it. You boost your blood as much as you think you can get away with. You put on as much muscle as you can while not lowering your power/weight ratio.
Really this discussion could be about any top rider from those 15 years. The key differentiation in a group of talented riders who trained hard was how they responded to the program. It is something that the doctors and DS' were well aware of at the time. It is also something that is found in most discussions of PED's in others sports. Some athletes, like Ben Johnson, Kelli White, etc. respond far better to doping then others.
Again, this sounds like unsupported speculation to me. I'm sure some athletes do respond to PEDs more than others. But other than the fact that an athlete with a low natural HT can raise it more—pre-passport—than one with a high HT, there is very little hard information to allow one to conclude who is a high responder and who a low responder. E.g., some individuals respond better to a given dose of EPO than others, i.e., have a greater increase in RBCs. There are studies demonstrating this. But are there any studies which identify which riders respond better in this sense than others? Of course not, no active rider can ever participate in a study involving EPO. And even if we did have these data, we lack information, as I pointed out earlier, allowing us to say which athletes benefit most from a given level of RBCs. As discussed here a while back, the relationship between oxygen intake and power is complex and variable. IOW, it's quite conceivable that a high responder to EPO, in the sense of greater synthesis of RBCs, could be a low responder in terms of how much power increase results from greater oxygen intake. It isn't all a matter of muscle mass.
Just because a couple of riders and cycling analysts said he was the best talent of his generation yet never speculated as to why (which one has to with the type of doping being practiced at the time), that doesn't take into account his absolutely abysmal form the large majority of the time he raced.
Seven TDF podia in ten years? That is abysmal form? Much has been said about the large margins of victory of LA in most of his Tours. Much less has been said about the large margins Ulle usually had over the third place finisher. If LA had been busted in '99 for corticosteroids, as he should have been, Ulle would have gone down as one of the great GT riders of all time. Yes, even after Puerto. I'm not arguing that he should have or shouldn't have, but just that his palmares were definitely not abysmal.
He was hounded out of the sport, yet he could have served a suspension with plenty of time to come back and redeem himself. He chose not to.
I was a little surprised by that, too. But by the time he came back he would have been at an age, mid 30s, when riders very rarely win Tours. I don't think after all the bridesmaid years he was interested in more podium finishes.
All three have one thing in common-ridiculous performances that announced to the cycling world "I'm here, I'm on dope, and no one can stop me"-Ullrich at Arcelis, Indurain's time trial from Tours to Blois, and Armstrong at Sestriere. I see no difference between these three performances.
Who wasn’t on dope at that time? To explain how LA won seven TDFs, the argument is that he had a better program, guided by Ferrari, than anyone else, supplemented by protection by UCI. With Ulle, it seems that some are now trying to make the case that he just responded better than others. All of this is useful speculation, but let's not delude ourselves into believing that we have a lot of hard evidence to support it. In LA's case, we have some evidence of protection, but no evidence yet that he used anything not available to others. We really have no direct evidence at all that Ulle's success was due to being a high responder.
- Aug 13, 2009
- 12,854
- 2
- 0
Merckx index said:20%?! In the nineties, maybe, but not after the EPO test.
what % is it when you increase from 39% to 50% ?
You are basing your assumption on one 3rd hand quoteMerckx index said:But based on the information I've seen, neither Ulle's nor LA's HT was exceptionally low.
Merckx index said:You seem to be implying that the program was tailored to coordinate the increase in muscle mass with an increase in oxygen intake. I doubt very much that the doping doctors were trying to do this, or that in fact one could do it.
And you would be wrong. It was one of the key parts of almost every top doping program of the 90's/00. No surprise that when Armstrong started working with Ferrari he showed up at training camp looking like a linebacker. Did you watch cycling in the 90's? Ever wonder how rider went full gas on climbs with their mouths closed, breathing out their nose?
Over the last several decades I have had many, many, many discussions about this topic with the doctors, directors, and riders you might have read about in the magazines. For them none of what I have written would be new.
- Aug 13, 2009
- 12,854
- 2
- 0
Zam_Olyas said:Will anyone tempt to answer this?
This deserves it's own thread
- May 26, 2010
- 28,143
- 5
- 0
Zam_Olyas said:Will anyone tempt to answer this?
I think we will never know. You could try and base possible winners on Vo2 Max and natural HCTs etc but it would be taking out the actual racing aspect and without that it would be a guessing game.
- Aug 13, 2009
- 12,854
- 2
- 0
Benotti69 said:I think we will never know. You could try and base possible winners on Vo2 Max and natural HCTs etc but it would be taking out the actual racing aspect and without that it would be a guessing game.
True.
EPO effectively killed the pure climbers who for decades were some of the key animators of Grand Tours. Even if we had an idea of who might have done better with a level playing field it would be hard to predict how the tactics would have changed
- Apr 7, 2011
- 4,887
- 465
- 16,580
Race Radio said:True.
EPO effectively killed the pure climbers who for decades were some of the key animators of Grand Tours. Even if we had an idea of who might have done better with a level playing field it would be hard to predict how the tactics would have changed
I guess you mean the likes of Pantani and Jiminez
- Mar 4, 2010
- 1,826
- 0
- 0
Merckx index said:And during a GT, much of the transfusion goes just to reverse the normal decline in HT
Which is due to volume expansion.
- Jun 25, 2009
- 305
- 0
- 9,280
Bavarianrider said:I guess you mean the likes of Pantani and Jiminez
EPO enabled big guys to climb with the climbers. The climbers coud not keep up on tempo/time trials. That's where they were killed, while their climbing weapon was neutralized.
- Dec 27, 2010
- 6,674
- 1
- 0
Trond Vidar said:EPO enabled big guys to climb with the climbers. The climbers coud not keep up on tempo/time trials. That's where they were killed, while their climbing weapon was neutralized.
That doesn't account for the doping climbers who were suddenly greatly improved timetriallists such as Basso, Heras, Mayo etc.
- Apr 7, 2011
- 4,887
- 465
- 16,580
Trond Vidar said:EPO enabled big guys to climb with the climbers. The climbers coud not keep up on tempo/time trials. That's where they were killed, while their climbing weapon was neutralized.
So Epo only made the "big guys" faster but not the climbers?

- Aug 13, 2009
- 12,854
- 2
- 0
Bavarianrider said:So Epo only made the "big guys" faster but not the climbers?
It is clear you do not understand how Oxygen vector doping works or it's effect on tactics. Yes, larger riders received greater benefit from EPO. It also turned huge portions of the peloton into climbers, neutralizing the attacks of climbers that once shattered the field. By 1989 less then 5 riders had broke 45 minutes on Alp d'Huez......in 1997 60 riders broke 45.
TRENDING THREADS
-
 Itzulia Basque Country 2026, April 6-11
Itzulia Basque Country 2026, April 6-11- Started by Dazed and Confused
- Replies: 977
-
 Ronde van Vlaanderen 2026, monument, April 5 (men's)
Ronde van Vlaanderen 2026, monument, April 5 (men's)- Started by Krzysztof_O
- Replies: 1K
-

-
 Teams & Riders The Remco Evenepoel is the next Eddy Merckx thread
Teams & Riders The Remco Evenepoel is the next Eddy Merckx thread- Started by DNP-Old
- Replies: 39K
-
 Teams & Riders Tadej Pogačar discussion thread
Teams & Riders Tadej Pogačar discussion thread- Started by Lequack
- Replies: 43K
-
 Milan San Remo, March 21, 2026, 298 km monument
Milan San Remo, March 21, 2026, 298 km monument- Started by topcat
- Replies: 1K
-


Cyclingnews is part of Future plc, an international media group and leading digital publisher. Visit our corporate site.
© Future Publishing Limited Quay House, The Ambury, Bath BA1 1UA. All rights reserved. England and Wales company registration number 2008885.